
Back in December, Serious Medicine Strategy took admiring note of an extraordinary medical operation that took place in New York City earlier that month. A team of surgeons led by Dr. Jean Emonds andDr. Tamoaki Kato performed a 43-hour ex vivo operation on Robert Collison, a Wisconsin man suffering from advanced and rampant cancer. In the ex vivo procedure, Collison's organs were removed, the cancer cut away, and then the organs were put back into Collison's body.
Now, sadly, five months later, Collison has died, as reported by The New York Times' Denise Grady, who has been following this case closely.
For his part, Dr. Emond, one of the team leaders at NewYork-Presbyterian/Columbia University Medical Center, said that the procedure would continue:
Dr. Emond said he expected the team in New York to continue performing ex vivo operations, even though health care “bean counters will be appalled at our profligate ways.” New York-Presbyterian/Columbia is a teaching and research hospital, he said, and part of its mission is to be innovative.
He said ex vivo surgery was still in its early days, and the team hoped to improve it to help patients like Mr. Collison.
“We’re not the kind of people who would stop,” Dr. Emond said.
And the truth, of course, is that everything is expensive and difficult at first. It only gets easier, and better, and cheaper, with practice.
But here's a prediction, the "bean counters" that Dr. Emond warns about will descend on this case, citing the expense--nearly $300,000, according to the Times--as an instance to be made into an example. This case could become a rallying cry for deficit cutters. Unfortunately, those deficit cutters don't see that a) such medical heroism is popular, and b) such medical heroism is also the beginning of a new industry.
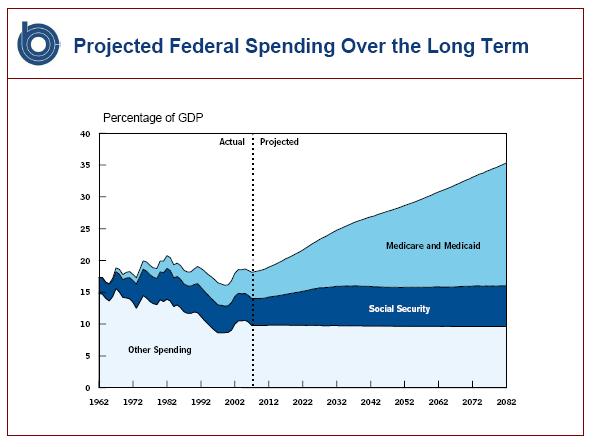
As it happens, Tuesday. April 27 is also the day that the deficit commission holds its first formal meeting in Washington. There will be much talk about Medicare spending as the biggest driver of entitlement spending, which, of course, it is. And there will be much talk about restraining the growth of Medicare. But there will be little practical effect, because all the approaches being talked about--deep cuts, in some form or fashion--are deeply unpopular. One of the deficit commission co-chairs, former Sen. Alan Simpson, calls it a "suicide mission." In so saying, Simpson helps to cement his reputation for both candor and courage, but we might note that what's really needed is vision and effectiveness. That is, in the long run it doesn't do much good to simply describe a problem--what matters is fixing the problem.
What might be popular is a larger look at Medicare spending, in which ways to make people healthier are explored. Good health is cheaper than bad health. To cite an obvious example, vaccines are cheaper than the disease, outpatient procedures are cheaper than inpatient procedures, and pills are ultimately cheaper than just about anything else. But getting to the point where life-saving and life-enhancing procedures are possible is a great challenge. As with good writing, it takes a lot of work to make it look easy.
And there's even a place for ex vivo surgery in that future Medicare plan. Because while ex vivo might seem expensive, there are plenty of people who would happily pay the $300,000 for the operation--or a lot more than that. And over time, not only would lives be saved, but a new economic engine for New York City and other medical hubs would develop.

We all know that we the American people who adamantly opposed this bill and whose voice was not heard are facing something out of Grimm's Fairy tales in the event this bill is not reworked. Right out of the shoot the bill is found to contain both financial and material errors. Revisions are being contemplated in some of the sugsr coated provisions that attracted so many unknowing citizens. Making revisions as we go along and suffering the slings and arrows of outrageous misfortune is not the right way to handle this can of worms. Practically nothing on the horizon conforms with how the bill was laid out marginally. I will never forget the Speaker telling us that we would find out what is in the bill after it was passed. Many politicians did not know either, many never read it. The talk on the street was that the Democrats and the Left just wanted something to push through. As far as R&D and search for the cure concerning our friend Michael J. Fox, if something is not done to revise this bill from the get go he will be lobbying for his cure into perpetuity.
ReplyDeleteThe blog you have just read above was written on May 2. As a futurist I guess I am never going to be able to put my shoulder to wheel. I was actually too benign in my original blog as we are beginning to see mayhem as of July. Now we see countless lawsuits and financial calculations that have elevated dramatically from the inception, angry doctors all over the country and some of the provisions in the bill itself which are in a quandary. A large segment of American citizens never wanted this bill to become law from the beginning. I may improve my crystal ball instincts by simply saying that I do not think that this form of healthcare is going to fly.
ReplyDelete